VIDAS® NT-proBNP2
Exclusion or Confirmation of Acute Heart Failure
VIDAS® NT-proBNP2 is a useful tool for rapid and clinical assessment and diagnosis of patients with symptoms of suspected heart failure.
High sensitivity and specificity allows initiation of timely, appropriate treatment.
Cost-effective tool adapted to emergency situations.
Disclaimer: Product availability varies by country. Please consult your local bioMérieux representative for product availability in your country.

- Overview
- Assay
- Resources
Overview
VIDAS® NT-proBNP2 (PBN2) is an automated quantitative test for use on the instruments of the VIDAS® family for the determination of N terminal fragment of Brain‑type natriuretic peptide in human serum or plasma (lithium and sodium heparin) using the ELFA technique (Enzyme-Linked Fluorescent Assay). The VIDAS® NT‑proBNP2 test is used as an aid in the diagnosis of suspected heart failure.1
Clinical Utility of VIDAS® NT-proBNP2
International guidelines recommend the use of B-type natriuretic peptide testing in the diagnostic workup of Heart Failure (HF) in both acute and non-acute patient presentation.2
NT-proBNP is indicated by International Guidelines1 as an aid in the diagnosis of individuals suspected of having congestive heart failure and detection of mild forms of cardiac dysfunction.
The test also aids in the assessment of heart failure severity in patients diagnosed with congestive heart failure. This assay is further indicated for the risk stratification of patients with acute coronary syndrome and congestive heart failure2, and it can also be used for monitoring the treatment in patients with left ventricular dysfunction.
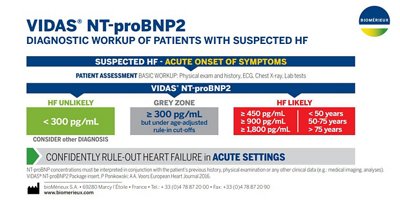
In the emergency department (ED), NT-proBNP is particularly useful for the triage of patients with acute dyspnea and suspected acute HF. It is highly sensitive and specific for exclusion (single rule-out cut-off value of 300 pg/mL) or confirmation of acute HF (age-adjusted rule-in cut-off values).3
In primary care, NT-proBNP is particularly useful to guide referral of symptomatic chronic HF to specialist care because it excludes suspected left ventricular systolic dysfunction. Compared with NT-proBNP values in patients with acute HF, lower values are expected in ambulatory chronic HF patients. International guidelines recommend a single low cut-off of 125pg/mL to rule out HF for patients presenting with non-acute symptoms. However, peer-reviewed literature supports the use of age-dependent cut-offs to adjust for loss of specificity in such settings.5
VIDAS® NT-proBNP2 is a useful tool offering:
- High sensitivity and specificity
- Initiation of timely, appropriate treatment
- Cost-effectiveness
- Adapted to emergency situations
Heart Failure
Heart failure (HF) is a complex clinical syndrome in which the heart's ability to pump blood is inadequate to meet the metabolic needs of the body. The most common symptoms are shortness of breath, fatigue, tachycardia, and edema.1
The natriuretic peptides, ANP (atrial natriuretic peptide), BNP (B for brain-type), and CNP (C-type natriuretic peptide) are neurohormones released from the heart (ANP and BNP) or vascular endothelial cells (CNP) in response to hemodynamic stress. They are involved in the regulation of intravascular homeostasis: vasodilation (antagonism of the renin-angiotensin system), natriuresis (increased renal sodium secretion), and diuresis.2
BNP and NT-proBNP concentrations in blood are well correlated but NT-proBNP levels are higher than BNP due to differences in half‑life (120 vs. 60 minutes).2 The kidneys equally clear both molecules, but BNP is also cleared by natriuretic peptide receptors or neutral endopeptidases (proteolysis).3 Elevated levels of NT-proBNP are associated with ventricular dysfunction and severity of HF.4 NT-proBNP also detects mild HF and HF with preserved ejection fraction.5,6
B-type natriuretic peptides are recommended in professional guidelines for the diagnostic evaluation of patients with acute dyspnea and suspected acute HF, particularly when the clinical diagnosis is uncertain.1,7 Studies have shown that inclusion of NT‑proBNP in diagnostic strategies of emergency department patients with suspected HF led to a reduction in time to discharge and costs.8,9 For diagnosis of acute HF, a single rule-out and multiple age‑dependent rule‑in cut‑off values have been established for NT‑proBNP in the ICON Study.10 European Society of Cardiology (ESC) guidelines include natriuretic peptide testing as a part of essential initial investigations for diagnosis of HF; i.e.as a screening tool in acute and chronic settings to exclude (rule out) HF and identify patients who require further investigations to confirm the diagnosis (rule-in).1 In the ambulatory (chronic) setting the ESC recommended NT-proBNP cut-off for HF exclusion is 100 pg/mL, whereas this is 300 pg/mL in the acute setting.11 In the acute setting, multiple age-dependent rule-in cut-off values have also been established for NT-proBNP: >450 pg/mL if aged <55 years, >900 pg/mL if aged between 55 and 75 years and >1800 pg/mL if aged >75 years.12
A proper differential diagnosis is important, because NT-proBNP is also elevated in other conditions affecting ventricular function such as pulmonary embolism, hypertension, valvular heart disease, muscle heart disease, arrhythmias, critical illness (for example, sepsis), anemia, and stroke.13
In primary care, NT-proBNP is particularly useful to guide referral of symptomatic chronic HF to specialist care because it excludes suspected left ventricular systolic dysfunction.14
NT-proBNP has independent prognostic value in a variety of clinical settings, including acute dyspnea with or without acute HF, chronic HF, stable and unstable ischemic heart disease.15, 16, 17 NT‑proBNP has incremental prognostic value in acute coronary syndromes with normal troponin.18
NT‑proBNP is a useful marker for inpatient monitoring in acute destabilized HF and therapy guidance in chronic HF.19, 20 The VIDAS® NT-proBNP2 assay contains two monoclonal antibodies which recognize epitopes located in the N‑terminal part (1‑76) of proBNP (1‑108).
VIDAS® Solutions
- Reliable and easy-to-use instruments with random access and small footprint.
- Well adapted to rapid response laboratories.
- Factory-calibrated, single-dose tests which reduce the need for additional controls.
- Short time to result.
- Reagents can be used immediately after removal from the refrigerator.
References
1. McMURRAY JJ, et al., ESC Committee for Practice Guidelines. ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: The Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2012;33:1787-847.
2. DANIELS LB, MAISEL AS. Natriuretic peptides. J Am Coll Cardiol. 2007;50:2357-68.
3. VAN KIMMENADE RR, JANUZZI JL JR, et al. Renal clearance of B-type natriuretic peptide and amino terminal pro-B-type natriuretic peptide a mechanistic study in hypertensive subjects. J Am Coll Cardiol. 2009;53:884-90.
4. KIM HN, JANUZZI JL Jr. Natriuretic peptide testing in heart failure. Circulation. 2011;123:2015-9.
5. EMDIN M, PASSINO C, et al. Comparison of brain natriuretic peptide (BNP) and amino-terminal ProBNP for early diagnosis of heart failure. Clin Chem. 2007;53:1289-97.
6. O'DONOGHUE M, CHEN A, et al. The effects of ejection fraction on N-terminal ProBNP and BNP levels in patients with acute CHF: analysis from the ProBNP Investigation of Dyspnea in the Emergency Department (PRIDE) study. J Card Fail. 2005;11(Suppl.):S9-14.
7. HUNT SA, et al. 2009 focused update incorporated into the ACC/AHA 2005 Guidelines for the Diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation. 2009;119:e391-479.
8. MOE GW, HOWLETT J, et al.; Canadian Multicenter Improved Management of Patients With Congestive Heart Failure (IMPROVE-CHF) Study Investigators. N-terminal pro-B-type natriuretic peptide testing improves the management of patients with suspected acute heart failure: primary results of the Canadian prospective randomized multicenter IMPROVE-CHF study. Circulation. 2007;115:3103-10.
9. RUTTEN JH, STEYERBERG EW, et al.. N-terminal pro-brain natriuretic peptide testing in the emergency department: beneficial effects on hospitalization, costs, and outcome. Am
Heart J. 2008;156:71-7.
10. JANUZZI JL, VAN KIMMENADE R, et al. NT-proBNP testing for diagnosis and short-term prognosis in acute destabilized heart failure: an international pooled analysis of 1256
patients: the International Collaborative of NT-proBNP Study. Eur Heart J. 2006;27:330-7.
11. McDONAGH T, et al. ESC Scientific Document Group. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021; 42:3599-3726.
12. JANUZZI Jr JL, CHEN-TOURNOUX AA, Christenson CHRISTENSON RH, et al, ICON-RELOADED Investigators. N-Terminal pro-B-type natriuretic peptide in the emergency department: The ICON-RELOADED Study. J Am Coll Cardiol. 2018; 71:1191-1200.
13. BAGGISH AL, VAN KIMMENADE RR, JANUZZI JL JR. The differential diagnosis of an elevated amino-terminal pro-Btype natriuretic peptide level. Am J Cardiol. 2008;101(Suppl).:43A-8A.
14. HILDEBRANDT P, COLLINSON PO, et al. Age-dependent values of N-terminal pro-B-type natriuretic peptide are superior to a single cut-point for ruling out suspected systolic dysfunction in primary care. Eur Heart J. 2010;31:1881-9.
15. BAGGISH AL, VAN KIMMENADE RR, JANUZZI JL Jr. Amino-terminal pro-B-type natriuretic peptide testing and prognosis in patients with acute dyspnea, including those with acute heart failure. Am J Cardiol. 2008;101(Suppl.):49A-55A.
16. MASSON S, LATINI R. Amino-terminal pro-B-type natriuretic peptides and prognosis in chronic heart failure. Am J Cardiol. 2008;101 (Suppl.):56A-60A.
17. OMLAND T, DE LEMOS JA. Amino-terminal pro-B-type natriuretic peptides in stable and unstable ischemic heart disease. Am J Cardiol. 2008;101(Suppl.):61A-6.
18. WEBER M, BAZZINO O, et al. N-terminal B-type natriuretic peptide assessment provides incremental prognostic information in patients with acute coronary syndromes and normal troponin T values upon admission. J Am Coll Cardiol. 2008;51:1188-95.
19. BETTENCOURT P, JANUZZI JL Jr. Amino-terminal pro-Btype natriuretic peptide testing for inpatient monitoring and treatment guidance of acute destabilized heart failure. Am J Cardiol. 2008;101(Suppl.):67A-71A.
20. PORAPAKKHAM P, PORAPAKKHAM P, et al. B-type natriuretic peptide-guided heart failure therapy: A meta-analysis. Arch Intern Med. 2010;170:507-14
Assay
Technical Specifications
| Assay | Reference | Tests per Kit | Code | Time to Results | Measuring Range |
|---|---|---|---|---|---|
| VIDAS® NT-proBNP2 | 30458 30458-30 | 60 tests 30 tests | PBN2 | 20 minutes | 15-25,000 pg/mL |
BECAUSE IT MAKES SENSE ON VIDAS®

Resources